FINAL EXAMINATION SHORT CASE
A 22 YEAR OLD MALE WITH PANCREATIC PSEUDOCYST
This is an online E log book to discuss our patient's de-identified health data shared after taking her guardian's signed informed consent.
Name : SOWJANYA REDDY PALAKURTHY
Hall Ticket Number : 1701006175
Roll no. - 130
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.This E-log also reflects my patient-centered online learning portfolio and your valuable inputs in the comment box are welcome.
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, Clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT : An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references.
DOA: 7/6/2022
A 22yr old male patient, painter by occupation , resident of nalgonda came with
CHIEF COMPLAINTS:
Pain abdomen since 4 days.
HISTORY OF PRESENTING ILLNESS:
5 YEARS AGO
Pt. Has started consuming alcohol 4 yrs back due to peer pressure , intially taking one peg per day which has increased to 90ml morning and evening i. e twice daily. He has stopped consuming alcohol 3 months back as advised by the doctor.
2 YEARS AGO
Pt. Has history of smoking since 2 yrs . He has been smoking 5 beedis/per day till date.
3 MONTHS AGO
Pt was apparently asymptomatic 3 months back then he developed abdominal pain which was dragging in character for which he was admitted in near by hospital in nalgonda . He was diagnosed with acute pancreatitis and was treated inadequately and was advised to stop consumption of alcohol.
Since then pt has stopped consuming alcohol and has been experiencing alcohol withdrawal symptoms like getting angry , agitation , irritability , craving to consume alcohol, tremors .
4 DAYS AGO
Pt had consumed alcohol 4 days back due to fight with his wife.
On 7/6/2022
In veiw of this symptoms pt.has been brought to psychiatry OPD for deaddiction. He was referred to medicine OPD in veiw of pain abdomen.
Pain was , insidious in onset , started after consuming of alcohol in epigastrium and left hypochondrium which was relieved on bending forward and lying down , aggregated on eating food and standing straight.
No h/o fever , nausea , vomiting, sweating.
No h/o Chest pain , shortness of breath , constipation
Flatus passed

PAST HISTORY:
H/o similar complaint in past 3 months back.
Not a known case of DM, HTN, BA, Epilepsy, TB.
No h/o previous surgeries
FAMILY HISTORY :
Insignificant
PERSONAL HISTORY
- DIET : mixed
- APPETITE : decreased
- BOWEL AND BLADDER: regular
- SLEEP: inadequate
GENERAL EXAMINATION :
Patient was examined in a well lit room. Henwas conscious, coherent and cooperative; Thin built and moderately nourished
Pallor - present

No icterus, cyanosis , clubbing, lymphadenopathy, edema
VITALS- at the Time of admission
- Temperature- afebrile
- Pulse rate- 94bpm
- Blood pressure-120/80mmHg
- Respiratory rate- 16cpm
SYSTEMIC EXAMINATION

1. ABDOMINAL EXAMINATION
Inspection:
- Shape of the abdomen- flat
- Umbilicus is central
- No visible scars,pulsations, peristalsis, engorged veins
Palpation:
- All the inspectory findings are confirmed.
- No local rise of temperature
- Tenderness present over the epigastrium and left hypochondrium region
- Liver palpable 2cms below costal margin
- Liver span: 11.5cm ( normal)
- Spleen : not palpable
- Kidney : not palpable
Percussion:
- No free fluid
Auscultation:
- Bowel sounds heard
2. RESPIRATORY SYSTEM - Normal vesicular breath sounds heard
3. CVS : S1 S2 heard , no added murmurs
4. CNS : Higher function intact ,No motor and sensory deficit, Cranial nerves normal .
INVESTIGATIONS:
1. USG ABDOMEN:

2. SERUM LIPASE : increased to more than three times - 112 IU/L
3. SERUM AMYLASE-255 IU/L
4. HEMOGRAM:

5. RANDOM BLOOD SUGARS: 97mg/dl
6. RENAL FUNCTION TESTS:

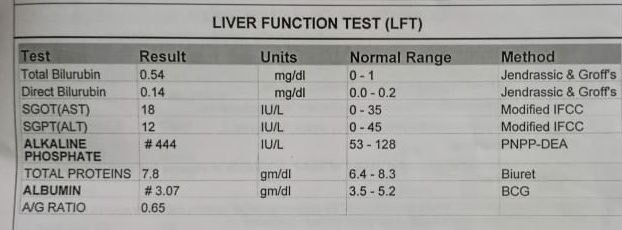
7. LIVER FUNCTION TESTS:
8. BLOOD GROUPING: O+ve
DIAGNOSIS
Pseudocyst of pancreas secondary to unresolved acute pancreatitis.
TREATMENT:
- Nil per oral (NPO)
- IV fluids RINGER LACTATE ,Normal saline 100 ml per hour
- Inj. TRAMADOL 100mg in 100ml NS IV BD
- Inj. PANTOP 40 mg IV OD
- Inj. OPTINEURIN 1 ampoule in 100ml NS IV OD
Psychiatric Medications
- Tab . Lorazepam 2mg BD
- Tab . Benzothiamine100mg OD