70 YEAR OLD FEMALE WITH DROWSY STATE
A 70 YEAR OLD FEMALE WITH URAEMIC ENCEPHALOPATHY + PRE-RENAL AKI
- 17th February 2022
This is an online E log book to discuss our patient's de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.This E-log also reflects my patient-centered online learning portfolio and your valuable inputs in the comment box are welcome.
SOWJANYA REDDY PALAKURTHY
ROLL NO. : 130
9th Semester
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, Clinical findings, investigations and come up with a diagnosis and treatment plan.
CASE:
A 70 year old female home maker since 10-15 years (farmer by occupation) came to the casualty in a drowsy state.
HOPI:
Patient was apparently asymptomatic 10 years back ,then patient had h/o fall for which she went to local hospital where she got diagnosed with Diabetes mellitus and since then she is on OHA medication (glim m2)
4 YEARS BACK
She had h/o fall and went to hospital and got diagnosed with HTN.
1 session of dialysis was done (indication/cause unknown)
1 MONTH BACK
she developed hypoglycaemia, secondary to OHA’s ,which was resolved later.
4 DAYS BACK
Patient had h/o fall 4 days back ,diagnosed as intertrochanteric fracture of femur of right leg, which was operated(CRIF done).
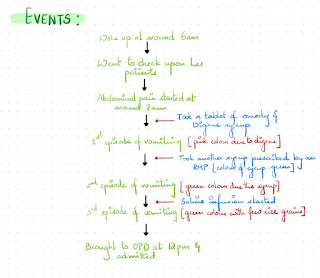
3 episodes of non-bilious, projectile vomiting associated with abdominal distension and on/off fever two days ago.
On POD 2
Patient was drowsy ,opening eyes to deep pain.
PAST HISTORY:
K/C/O DM since 10 Years & on medication
K/C/O HTN since 4 Years
GENERAL EXAMINATION:
O/E : Patient is responding to vocal commands
- Pallor - present

- Icterus absent
- Cyanosis - absent
- Edema of feet - present


- Lymphadenopathy - absent
- Clubbing - absent
VITALS:-
- BP: 170/90mmhg
- PR: 98 bpm
- RR: 25cpm
- Spo2: 95%
- Grbs: 146
SYSTEMIC EXAMINATION :
- CVS : S1 and S2 heard, no murmurs heard
- RS : BAE present
- P/A : soft
- CNS: Pt is drowsy.
- tone : normal
- Raised echogenecity in both kidneys.
- Multiple small calculi in Gallbladder.





8. SERUM CREATININE-

1. ABG-

2. RFT-

DAY 3 (14/02/2022)




DAY 5 (16/02/2022)
1. HEMOGRAM-

2. ABG-

3. RFT-

- No abnormality detected
- No features of Small Bowel Obstruction
- Left sided kidney- small
Uremic encephalopathy with pre renal AKI with POD 4 right femur fracture ? CRIF + PFM with DM and HT
TREATMENT:
On 12/2/22:
1. INJ. Lasix 40mg IV/BD
2. INJ. HAI SC/TID
3. INJ. CEFTRIAXON 1g/IV/BD
4. INJ. CLINDAMYCIN 600mg/ IV /TID
5.INJ. CLEXANE 20 mg SC/OD
6. INJ. OPTINEURON 1 AMP in 100 ml NS /IV/OD
7.TAB. Amlong 10mg PO /OD
8.IVF NS UO + 30 ml/hr
On 13/2/22:
1. INJ. Lasix 40mg IV/BD
2. INJ. HAI SC/TID
3. INJ. CEFTRIAXON 1g/IV/BD
4. INJ. CLINDAMYCIN 600mg/ IV /TID
5.INJ. CLEXANE 20 mg SC/OD
6. INJ. OPTINEURON 1 AMP in 100 ml NS /IV/OD
7.TAB. Amlong 10mg PO /OD
8.IVF NS UO + 30 ml/hr
On 14/2/22:
Vitals:
- TEMP: 101 F
- PR: 92bpm
- BP:-140/60mmhg
- GRBS: 123MG/DL
- CVS: S1S2 heard , no murmurs
- RS : BAE present
- P/A: GUARDING PRESENT
- I/O: 2400/2600
- Stools : not passed
Treatment:
- INJ. MONOCEF 1GM/IV/BD
- INJ. LASIX 40 MG IV/BD
- INJ. HAI SC/TID
- INJ. CLINDAMYCIN 600mg/ IV /TID
- INJ. CLEXANE 20 mg SC/OD
- TAB. Amlong 10mg PO /OD
- IVF NS UO+ 30ML/HR

On 15/02.2022
Vitals:
- TEMP:-98.4 F
- PR:-96 bpm
- BP: 150/ 90mmhg
- GRBS: 245MG/DL
- CVS:-S1S2 heard , no murmurs
- RS : BAE present
- P/A:-GUARDING PRESENT
- I/O: 2100/3200
- Stools : passed
Treatment:
- INJ. MONOCEF 1GM/IV/BD
- INJ. LASIX 40 MG IV/BD
- INJ. HAI SC/TID
- INJ. CLINDAMYCIN 600mg/ IV /TID
- INJ. CLEXANE 20 mg SC/OD
- TAB. Amlong 10mg PO /OD
- IVF NS UO+ 30ML/HR
- INJ ERYTHROPOIETIN 4000 IU/SC/WEEKLY ONCE
On 16/02/2022
- INJ. MONOCEF 1GM/IV/BD
- INJ. PIPTAZ 9.5 MG/ IV
- INJ. LASIX 40 MG IV/BD
- INJ. HAI SC/TID
- INJ. CLINDAMYCIN 600mg/ IV /TID
- INJ. CLEXANE 20 mg SC/OD
- TAB. Amlong 10mg PO /OD
- IVF NS UO+ 30ML/HR


On examination:
Pt is C/C/C
Abdominal pain - reduced
BP- 120/90 mmHg
PR- 96bpm
3 sessions of hemodialysis done
Investigations:
1. Hemogram:
- Hb-7.3
- TLC - 29,000
- PLT- 1.5
- D- DIMER - 3280
2. RFT
- UREA - 66
- SERUM CREATININE- 2.3
- URIC ACID-4.6
- Ca- 8.8
- PO4 - 4.2
- Na-139
- K- 3.3
- Cl- 90
- I/o - 2400/3000ml
Treatment:
- INJ: PIPTAZ 9.5 MG / IV
- INJ. LASIX 40 MG IV/BD
- INJ. HAI SC/TID
- INJ. CLINDAMYCIN 600mg/ IV /TID
- INJ. CLEXANE 20 mg SC/OD
- TAB. Amlong 10mg PO /OD
- IVF NS UO+ 30ML/HR

- Right IT femur fracture, CRIF + PFN DONE with DM + HTN
- 3 Sessions of hemodialysis done.
- Afebrile
- BP- 140/100 mm of Hg
- PR: 90 bpm
- CVS: S1 S2 +
- Respiratory system: BAE+
- PER ABDOMEN : Soft and tender
- Grbs : 8Am - 223mg/dl
- I/O: 1700/2100 ml
- INJ: PIPTAZ 9.5 MG / IV
- INJ. LASIX 40 MG IV/BD
- INJ. HAI SC/TID
- INJ. CLINDAMYCIN 600mg/ IV /TID
- INJ. CLEXANE 20 mg SC/OD
- TAB. Amlong 10mg PO /OD
- IVF NS UO+ 30ML/HR
- Inj Erythropoietin 4000IU/ SC / weekly once
- BP , PR, SPo2, temperature monitoring